


Let's talk about sudden cardiac death
Frank Han MD FAAP – Adult Congenital and Pediatric Cardiologist

Let’s sit down, around the fireplace, and actually talk properly about sudden cardiac death.
There is understandably, a great deal of anxiety surrounding the recent news reports in the past year of sudden cardiac arrests and sudden death in the media. Naturally, nefarious actors are using these reports for their own purposes, but just for the moment, I would like to share with you, how this analysis is conducted properly. Why am I qualified to speak about this? I am a pediatric and adult congenital cardiologist who has as one of his tasks, saving these sorts of patients and figuring out why it happened. I’ll take you from the granular view up to the 30,000 ft epidemiological view of how this subject should be treated professionally.
The first and most important step is prevention. None of us physicians like to see a sudden cardiac arrest, and should it happen - you, the reader, will witness someone drop and become unresponsive. The American Heart Association strongly recommends that Basic Life Support be initiated as soon as possible. There are a maze of reasons why people drop and become unresponsive, but the most helpful things a non-medical person can do are to preserve breathing, circulation, and the airway by performing chest compressions and using an Automated External Defibrillator. The chest compressions are meant to help the heart generate some circulation, and the defibrillator is programmed to give a high energy electrical shock to the patient should the reason for cardiac arrest be a useless electrical rhythm. If you remember nothing else from this article, remember this paragraph.
If we get the patient back, the patient will next need medical care and a certified consultant cardiologist or physician to think through the maze of reasons why the cardiac arrest occurred. Initial hospital care is going to revolve around stabilizing concurrent medical conditions, securing breathing, treating heart rhythm disorders, maintaining fluid status, and several other things depending on the actual situation at hand. If a cardiac cause of cardiac arrest is suspected, you will see the consultant cardiologist think through some of the causes listed in this article.
The testing that is usually done is some combination of an electrocardiogram (test of heart rhythm), echocardiogram (imaging the heart), and blood tests. Many times an answer is reached but other times, this requires more extensive testing outside the hospital. If a definite deadly heart rhythm is found, you will sometimes hear cardiologists recommend patients going home with a defibrillator to protect the patient from a deadly heart rhythm in the future.
If the patient actually died, then the next step is to perform a complete autopsy. While it is true that the United States has a shortage in fellowship trained pathologists, that topic is complex and serious enough that it deserves its own article. There are well-researched, professional guidelines for how to perform the cardiac autopsy. Pathology trainees spend entire sections of their training on how to do this correctly (although they may not necessarily choose to be employed by a coroner's office at the completion of their training). Pathology can reveal things like hypertrophic cardiomyopathy, significant heart artery blockages, myocarditis, dilated cardiomyopathy, and quite a few other things. It is a good autopsy combined with an accurate death certificate, that is going to provide the verified data for epidemiologists to use to figure out sudden deaths.
Once we figure out that there are sudden cardiac arrests, we must turn only to verified databases run by professional epidemiologists who source only verified data. Because the general news media (and unsavory sources) like to mix intense emotions into this subject - I strongly, strongly encourage the person curious about this subject to remove their emotions from the equation altogether. It is intense emotions that lead us astray from the professional analysis that is needed to actually get this subject straight. Do not reach for Peter McCullough, Stew Peters, Robert Malone, Rumble videos, cellphone videos of cellphone videos, or political pundits crying that there is censorship. It is the most charismatic charlatan who is the most effective at stirring up feelings for a cause despite the absence of evidence. A tiger made of paper is still a piece of paper.
With this knowledge under our belts we can now directly address the claim of whether or not there are increased sudden cardiac arrests due to the COVID immunizations.
A concept must be introduced to begin the analysis - excess death. Because death certificates and autopsies cannot be instantaneously conducted, there is a reporting delay. If in some future rendition of the US healthcare system there are Star Wars style robots that can instantly diagnose the cause of death, this may change. The excess death is a quantity of deaths that is above the average deaths in the same period during the year before. The deaths in the previous year are known, and can be tabulated by epidemiologists. The deaths in the current year are known but the investigator doesn’t know how they died. So, the epidemiologists reporting the current year’s data can report how the amount of deaths differs from the deaths in previous years. The results can be updated and categorized once actual causes of death are known.
With this knowledge, we can actually forge ahead to the real statistics provided by epidemiological agencies around the world.
We can make some general observations about excess deaths during the pandemic - both excess deaths (and confirmed deaths due to COVID) were definitely higher at multiple times, where some of those times correlated with COVID waves.

We can also look at EMS data showing the survival of out of hospital cardiac arrest, which worsened during the early part of the pandemic.
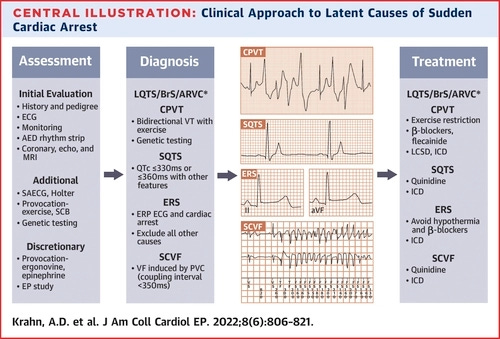
While we do not currently have the data for 2021-2022 in most countries, we do have historical references on examples of professionally done research that tabulates precisely, the adjudicated underlying causes of sudden cardiac arrest after all available medical records and death certificates were processed (Prospective Countywide Surveillance and Autopsy Characterization of Sudden Cardiac Death: The San Francisco Postmortem Systematic Investigation of Sudden Cardiac Death (POST SCD) Study (nih.gov)):

Total number of Rumble videos used? Zero. Total number of news reports claimed as verified statistics? Zero. Total number of claims of CDC censorship? Zero. Total number of pundits claiming all deaths are due to the COVID vaccine? Zero. This is how you actually sort this stuff out. The best journal article to analyze next would be the 2020-2022 equivalent of this project, however it is not done yet. Statisticians and epidemiologists are trying to figure out the causes of all the excess deaths during the COVID pandemic, but this requires effort and time.
The causes of excess death that have evidence so far include decline in healthy lifestyle choices, undiagnosed COVID, delays in routine care, delays in Emergency care (a stark example in 2023 is the British NHS), delayed deaths from other diseases, and the long term impacts of COVID at all severities. One thing that is quite well established now, is that COVID is capable of causing multiple organ system issues long after the initial COVID infection has resolved (This JAMA piece and this one from Nature are just two of many sources). Naturally, those who believe COVID vaccinations should be stopped around the world point to the cases of COVID immunization deaths due to myocarditis or a deadly arrhythmia (heart rhythm problem). The formal analysis of COVID immunization myocarditis is actually quite complicated due to the need to follow standardized autopsy guidelines, and the need for a systematic search for all plausible causes of myocarditis along with alternatives causes of death (other than myocarditis). The German Center for Infectious Disease Research put forth an admirable effort to show how to do such a comprehensive autopsy but, they alas did not perform molecular confirmation of active SARS-COV2 infection in the heart issue. In addition, international societies are seeing some heterogeneity in the characteristics of the myocarditis, so as of 2023, no consensus criteria are available apart from the systematic search for other pathogens with the exclusion of active SARS-COV2. One trend that can be discerned from the scattered case studies out there is - many of the decedents did not seek out medical care. So, please familiarize yourself with the symptoms of myocarditis and seek out medical care should you suspect them in the first month after immunization.
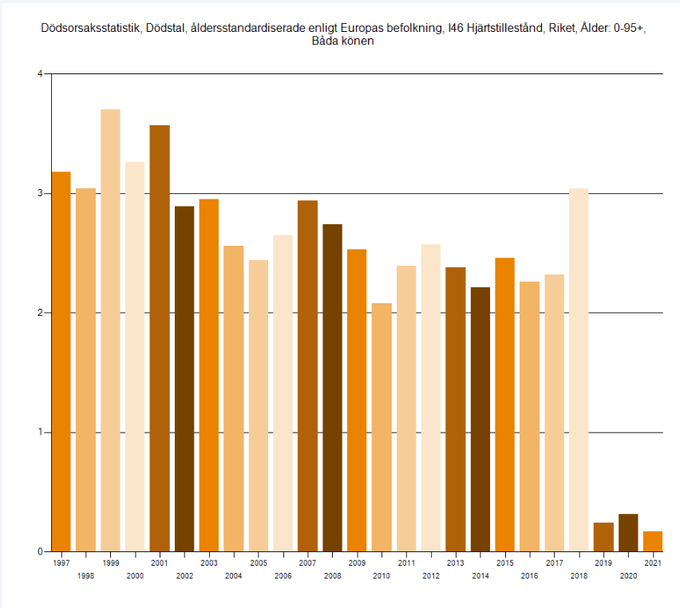
To address the question of whether or not people are dying at increased rates due to COVID immunization myocarditis, an analysis of an entire population must be discussed. The absolute and relative death rates of confirmed COVID immunization myocarditis are really small numbers compared to the total number of people who received immunizations, so large populations must be assessed to determine any true pattern. A country in which this can be analyzed is Sweden! They are one of the most vaccinated countries on the planet. They have lower baseline incidences of ischemic cardiovascular disease than the United States, which partially removes some of this confounding, yet in 2020-2021, they reported some of the lowest deaths due to sudden cardiac arrest in their entire history. If the parties hostile to COVID vaccination genuinely believe that COVID vaccinations cause excess sudden cardiac death across all age groups, then they owe us a logical explanation, with epidemiological proof, why this pattern was observed in Sweden. A related database in the United States is called CDC Wonder. A search can be done for all instances of myocarditis and sudden cardiac arrest in patients ages 15-44 in all regions of the US, once for 2019, and once for 202. The tabulated crude reporting rate is 0.4 per 100,000 in 2019, and 0.5 in 2020. The Covid vaccines became available in 2020 - and if there is a belief out there that there was a massive increase in myocarditis cases, the bits of data out there certainly don’t reflect that yet.
I look forward to professional epidemiologists sharing their eventual analyses of the 2021-2022 causes of excess sudden cardiac death in the worldwide population. Until then - please mitigate COVID as best you can, because everyone benefits. At the most basic level you won’t need to call out sick. At the most serious level - you might just avoid serious medical problems.
Excellent article, Dr. Han. Krahn et Al’s article was really good to think through causes of sudden arrhythmic death. There are many confounding problems with lack of available data. Look forward to a follow up article when epidemiological data more available. Thanks again.
Robbie Coltrane sadly died last year. I was trying to find out the cause of death and everything seems very strange, to say the least: it took 9 days for the information to be released. Then they said it was sepsis (if I am correct, sepsis is the final stage of an untreated infection, the name of the infection wasn't though mentioned). Then the uk newspapers seem to all repeatedly say how he struggled with a medical condition for the last 2 year, as though this could be the cause of death: artheritis - which obviously doesn't kill and it is a very common condition. What was the real cause of his death? (This is the first time I write to you and I am not quite sure where exactly to ask this question, I do apologise for placing it here)